
1. The Mirage of “Stabilized
At first glance, France’s 2024 national health data looks calm. HIV diagnoses appear stable. The numbers suggest control. Progress. Relief. But averages can hide danger.
When you look closer, you see something else. In certain neighborhoods, the pressure is rising. Bacterial sexually transmitted infections are increasing. Vulnerable communities are carrying a heavier load.
The virus may no longer dominate headlines. But for many families, the risk has not disappeared. It has changed. We are no longer fighting only infection. We are watching infection turn into a lifelong chronic disease.That is the real story.
2. The Six-Year Window: Where Migration Meets Risk
For years, many believed that HIV entered France through migration itself. That assumption is wrong. The ANRS Parcours study shows a different truth. Many Sub-Saharan migrants acquire HIV after they arrive. Let that sink in. Between 35% and 49% of Sub-Saharan migrants living with HIV were infected after arriving in France. Why? Because the first six years after arrival are often unstable.
• Housing is uncertain.
• Legal status takes time.
Work is insecure.
• Social isolation is real.
The average time needed to secure stable housing and residency? Six years. During this waiting period, 58% of post-migration infections occur. The biological risk window mirrors the administrative waiting period. This is not a coincidence. It is systems design. When people lack stability, risk rises. When legal protection is delayed, vulnerability grows. The virus does not create that instability. The system does.
3. HIV as an Accelerator: The Aging Shift
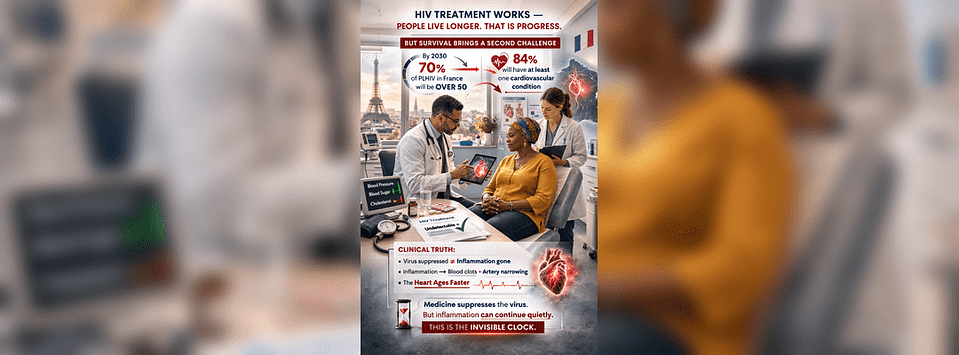
HIV treatment works. People live longer. That is progress. Survival is progress. But survival brings a second challenge. By 2030, 70% of people living with HIV in France will be over 50 years old. And 84% are expected to have at least one cardiovascular condition. Here is what the clinical data tells us: Even when HIV is controlled and undetectable, the body can remain in a state of chronic inflammation. That inflammation increases the risk of blood clots and artery narrowing. In simple terms: The heart ages faster. Medicine suppresses the virus. But inflammation can continue quietly. This is the invisible clock.
4. The Geography of Risk: Île-de-France

The Greater Paris region is where this pressure is strongest. Île-de-France holds a high concentration of migrant communities. It is also where housing instability and legal delays are most intense. Here, the six-year waiting period meets crowded housing and economic strain. Tuberculosis risk overlaps with immune stress. HIV overlaps with metabolic disease. What began as an infection becomes a cardiometabolic burden. The health system was built to treat viruses. It was not built to manage decades of chronic aging with infection. And the pressure is growing.
5. The Silent Multiplier: Hypertension

For many Sub-Saharan communities, hypertension is already common. In European studies, rates can reach 50% or more. Hypertension alone increases stroke and heart attack risk. Now add HIV. For people living with HIV, the risk of major cardiovascular events is 1.5 to 2 times higher. And the pressure does not stop there. Non-traditional risk factors multiply the danger:
• Economic insecurity
• Chronic stress
• Depression
• Substance use
• Drug interactions between HIV treatment and blood pressure medication
This is not about individual weakness. This is about layered risk. When stress, inflammation, and high blood pressure combine, the heart carries the cost.
6. The Weight of Prevention
Modern HIV treatment is life-saving. It is one of medicine’s greatest achievements. But some treatments can affect metabolism. Certain drug classes are linked to weight gain. Others can raise cholesterol or triglycerides. This weight gain is more pronounced in some Sub-Saharan populations. Let’s be clear: This is not about willpower. It is not about lifestyle failure. It is a biological response to treatment.
That means monitoring must be precise. If we do not track blood pressure, blood sugar, cholesterol, and weight carefully, the cure for the virus may inadvertently accelerate the progression to heart disease. Prevention is maintenance. And maintenance requires systems, not blame.
7. Beyond the Clinic: The Role of Community
Modern HIV treatment is life-saving. It is one of medicine’s greatest achievements. But some treatments can affect metabolism. Certain drug classes are linked to weight gain. Others can raise cholesterol or triglycerides. This weight gain is more pronounced in some Sub-Saharan populations. Let’s be clear: This is not about willpower. It is not about lifestyle failure. It is a biological response to treatment.
That means monitoring must be precise. If we do not track blood pressure, blood sugar, cholesterol, and weight carefully, the cure for the virus may inadvertently accelerate the progression to heart disease. Prevention is maintenance. And maintenance requires systems, not blame.
Housing is prevention. Legal security is prevention. Economic stability is prevention.
8. The Generational Question
Now we return to the central question: When an infectious disease becomes a chronic harm, who absorbs the long-term cost? HIV is no longer only an infectious issue. It is a test of how systems protect vulnerable people over time. Whether a migrant in France can expect a healthy 100-year lifespan depends less on the virus itself and more on what happens during those first six years. If we ignore that window, we do not stop the clock. We simply watch it run. And an entire generation pays the price.

Why Review The Biological Cost of Precarity?
Because instability affects more than circumstances — it affects the body. This presentation shows how housing insecurity, legal delays, and economic stress can lead to chronic inflammation, heart disease, and long-term harm. It connects policy to biology and shifts the focus from blame to systems. Understanding this link is essential for protecting health across generations.