



Series Five: The Caribbean Focus: Diabetes & Kidney Disease
Flagship Question: What does chronic disease reveal about health systems in majority-Black nations?
Introduction: The Unseen Crisis at the Table
In Caribbean homes, the kitchen has always been more than a place to prepare food. It is where memory lives. Where culture is passed hand to hand. Where elders teach, children learn, and love is expressed in seasoning, texture, and time. But today, something has quietly taken a seat at that table.
Across the Caribbean, families are living with a health crisis that does not arrive suddenly or dramatically. It does not spread from person to person. It settles in slowly—through food systems, work systems, and policy systems—until entire communities are managing illness as a way of life. Diabetes. Hypertension. Kidney disease.
These conditions now account for the majority of premature deaths across much of the Caribbean. In CARICOM states (excluding Haiti), non-communicable diseases are responsible for between 62% and 80% of all deaths, many occurring well before old age.
This is not a story about individual failure,It is not a story about “poor choices.”
It is a story about design.
This article is part of Afro Mosaic: Impacts on the Global Black Lifespan Journey—a 52-week investigation tracing Black life from birth to 100+ years through the intersecting forces of health, law, social structure, and economic power. In Series Five, the Caribbean becomes a critical checkpoint: a region where chronic disease reveals what happens when health systems are built to manage labour rather than sustain human life. The years being lost are not accidental. They are being structured away.
1. Health as Maintenance: The Afterlife of Plantation Medicine
To understand why diabetes and kidney disease dominate Caribbean health outcomes today, we must begin with a truth that predates modern public health. Caribbean medicine did not emerge from a philosophy of wellness.
It emerged from a philosophy of productivity.
On 18th- and 19th-century plantations, health was defined narrowly: the capacity of an enslaved person to work. Physicians were not healers in the modern sense. They were managers of human output. Enslaved Africans were described in medical and economic records as “human machinery,” “rational objects,” or “human motors”—assets whose value had to be preserved at the lowest possible cost.
This is where several enduring concepts were born:
- “Sick time” was not a benefit. It was a calculated pause, designed to minimize lost labor and restore productivity as quickly as possible.
- The plantation infirmary existed not to relieve suffering, but to return bodies to the field.
- A “cure” meant resuming work—not long-term health, not dignity, not flourishing.
White male physicians displaced African and Indigenous healers by claiming their methods reduced “days lost.” In doing so, they established a medical culture whose primary allegiance was not to the patient, but to the economic system. That logic did not disappear with emancipation. It evolved.
2. From Plantation Ledgers to Modern Health Systems
After slavery, the accounting practices used to track enslaved bodies—working days, sick days, depreciation—became templates for managing free labor. Modern health systems inherited this logic.
Across the Caribbean, chronic disease is often addressed not through early prevention, food systems reform, or environmental protection, but at the point of failure: dialysis units, amputations, late-stage complications.
This is not because prevention is unknown. It is because the system was never designed to prioritize it.
When healthcare is treated as a maintenance cost rather than a human right, investment flows toward keeping people functional enough to work—not toward protecting lifespan over decades. The result is a familiar pattern:
- Diabetes diagnosed late
- Kidney disease detected only at advanced stages
- Dialysis systems strained and centralized
- Families absorbing emotional, financial, and caregiving burdens
This is plantation logic in modern form: repair the worker when the machinery breaks.
3. The Hidden Bill: How Chronic Disease Drains Caribbean Futures
The cost of chronic disease is often discussed in hospital budgets and clinic shortages. But the true bill is much larger—and far more damaging. When people fall ill in their 40s, 50s, and 60s, entire economies absorb the shock.
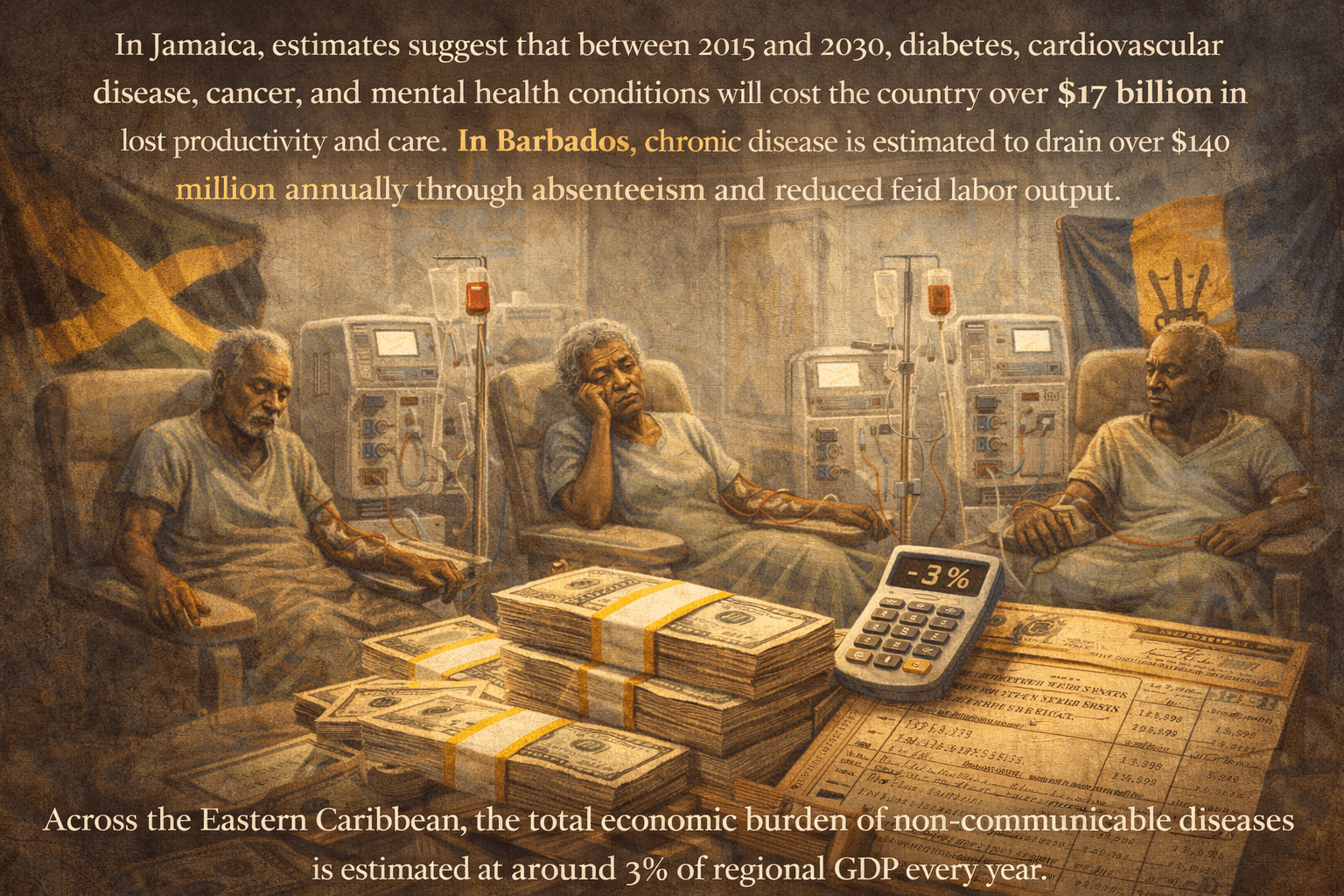
In Jamaica, estimates suggest that between 2015 and 2030, diabetes, cardiovascular disease, cancer, and mental health conditions will cost the country over $17 billion in lost productivity and care. In Barbados, chronic disease is estimated to drain over $140 million annually through absenteeism and reduced labor output.
Across the Eastern Caribbean, the total economic burden of non-communicable diseases is estimated at around 3% of regional GDP every year.
This is wealth that could be funding schools, climate resilience, food sovereignty, and elder care. Instead, it is being redirected to manage preventable illness.
This is not an unfortunate coincidence. It is a predictable outcome of policy choices.
4. The Battle of the Black Octagon: Why Food Labels Matter
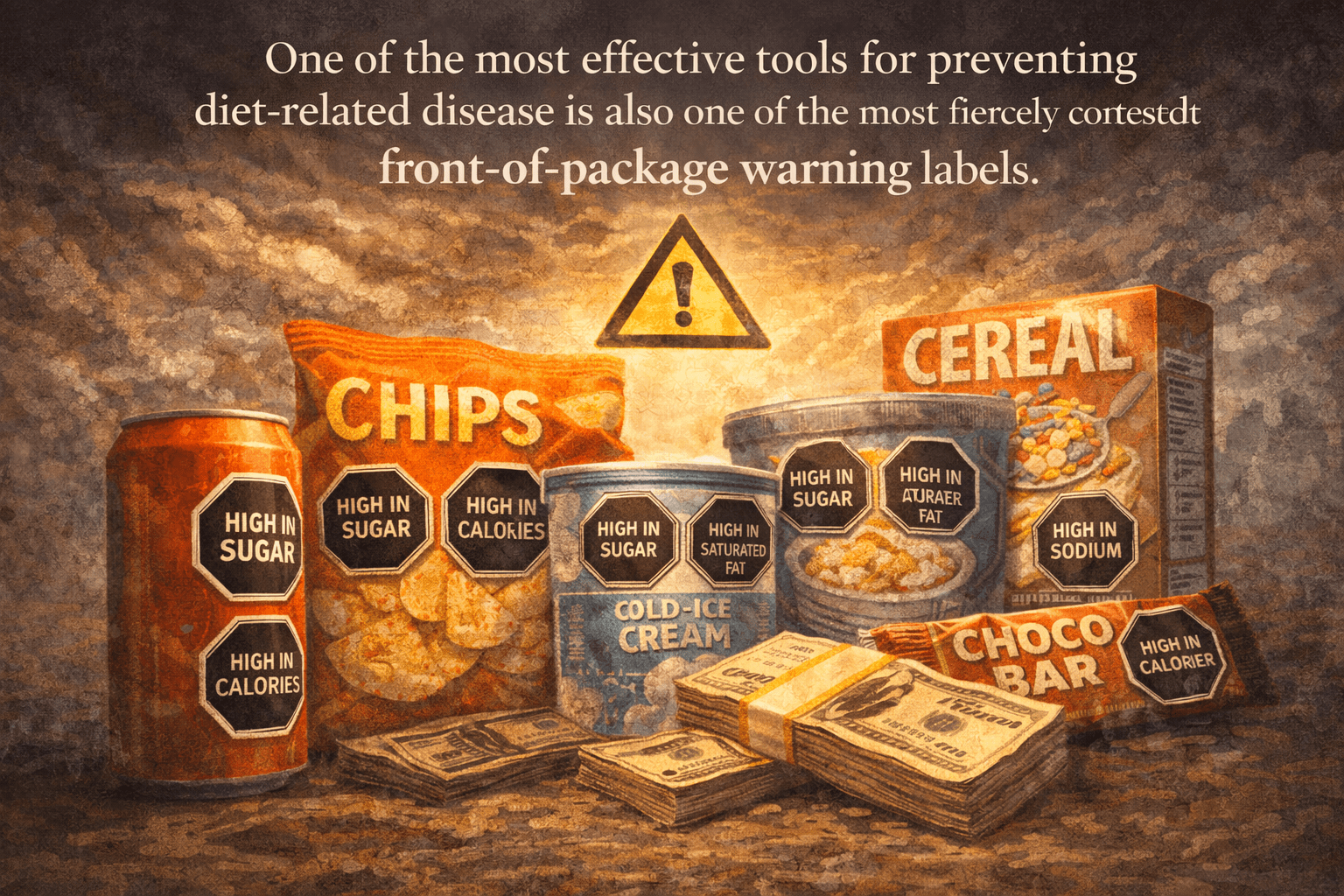
One of the most effective tools for preventing diet-related disease is also one of the most fiercely contested: front-of-package warning labels.
These labels—simple black octagons that read “High in Sugar,” “High in Salt,” or “High in Fat”—are designed to function like stop signs. They cut through marketing language, bright colors, and misleading claims to deliver one clear message: this product carries health risk. Decades of evidence show that these labels:
- Are quickly understood across literacy levels
- Reduce purchases of ultra-processed foods
- Encourage product reformulation
- Protect children and adolescents
For Caribbean families navigating imported food environments, they are not cosmetic. They are protective.And that is precisely why they have been resisted.
5. Corporate Resistance and the New Plantation Economy
The Caribbean food and beverage industry operates within a familiar logic: maximize throughput, minimize regulation, externalize health costs. When governments moved toward adopting clear warning labels, industry groups responded with a coordinated strategy:
- Commissioning alternative studies to create doubt
- Promoting “hybrid” labeling models that confuse rather than clarify
- Framing public health standards as trade barriers
- Warning of economic catastrophe without evidence
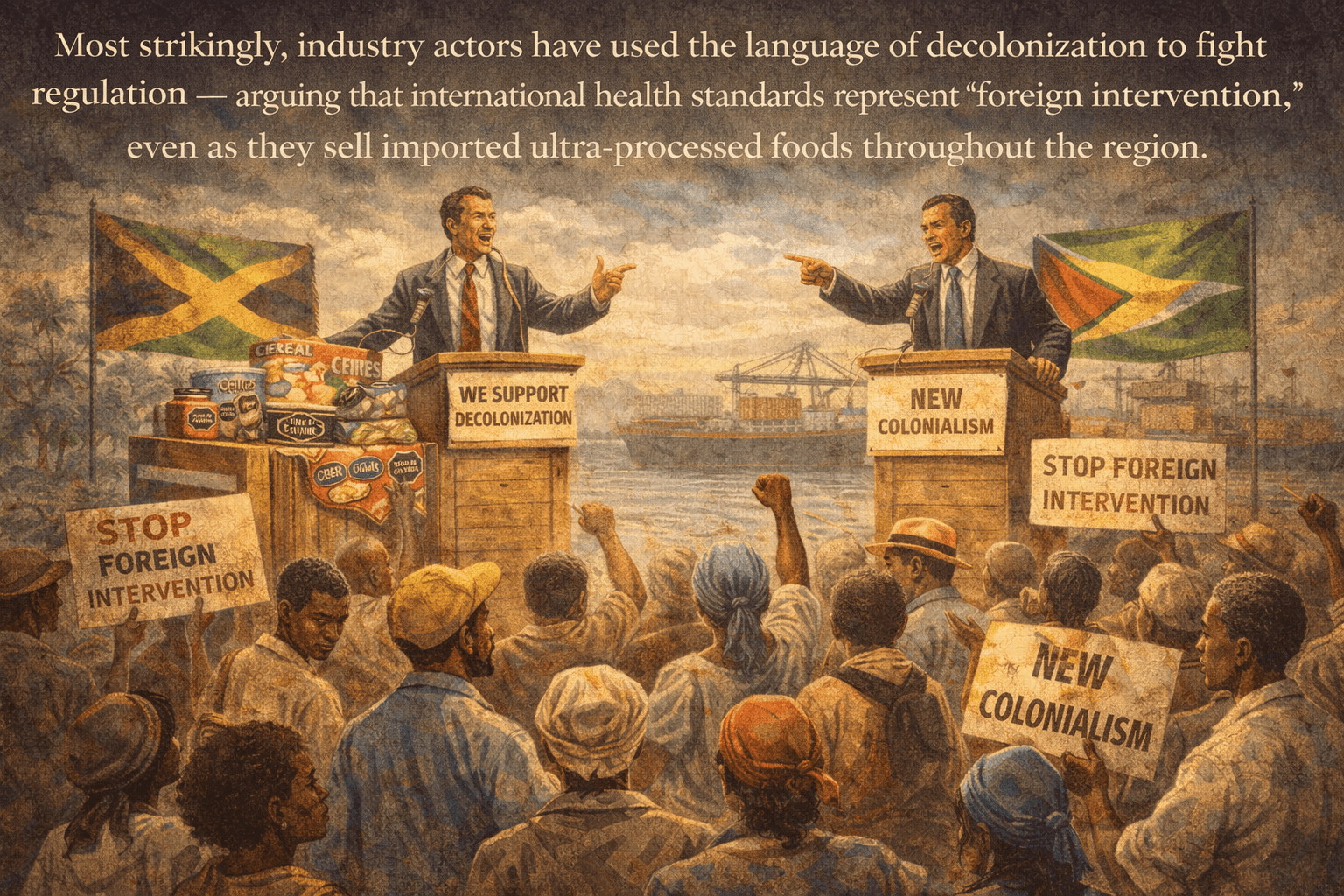
Most strikingly, industry actors have used the language of decolonization to fight regulation—arguing that international health standards represent “foreign intervention,” even as they sell imported ultra-processed foods throughout the region.
This is a profound inversion. The language of sovereignty is deployed not to protect Caribbean lives, but to protect corporate margins.
6. Jamaica and the Anatomy of a Policy Reversal
Nowhere was it more visible than in Jamaica.
Initially, expert committees, consumer advocates, and health professionals supported the adoption of strong warning labels. But following intense lobbying and an emergency meeting, positions shifted.
Votes were reversed. Processes became opaque. Consumer representatives withdrew support. To date, there has been no full public explanation.
What is clear is this: when health policy is decided behind closed doors, the people most affected lose their voice. This is not merely a procedural issue. It is a lifespan issue.
7. From Fields to Fries: How Trade Reshaped the Caribbean Diet
The modern Caribbean diet did not evolve organically. It was engineered.
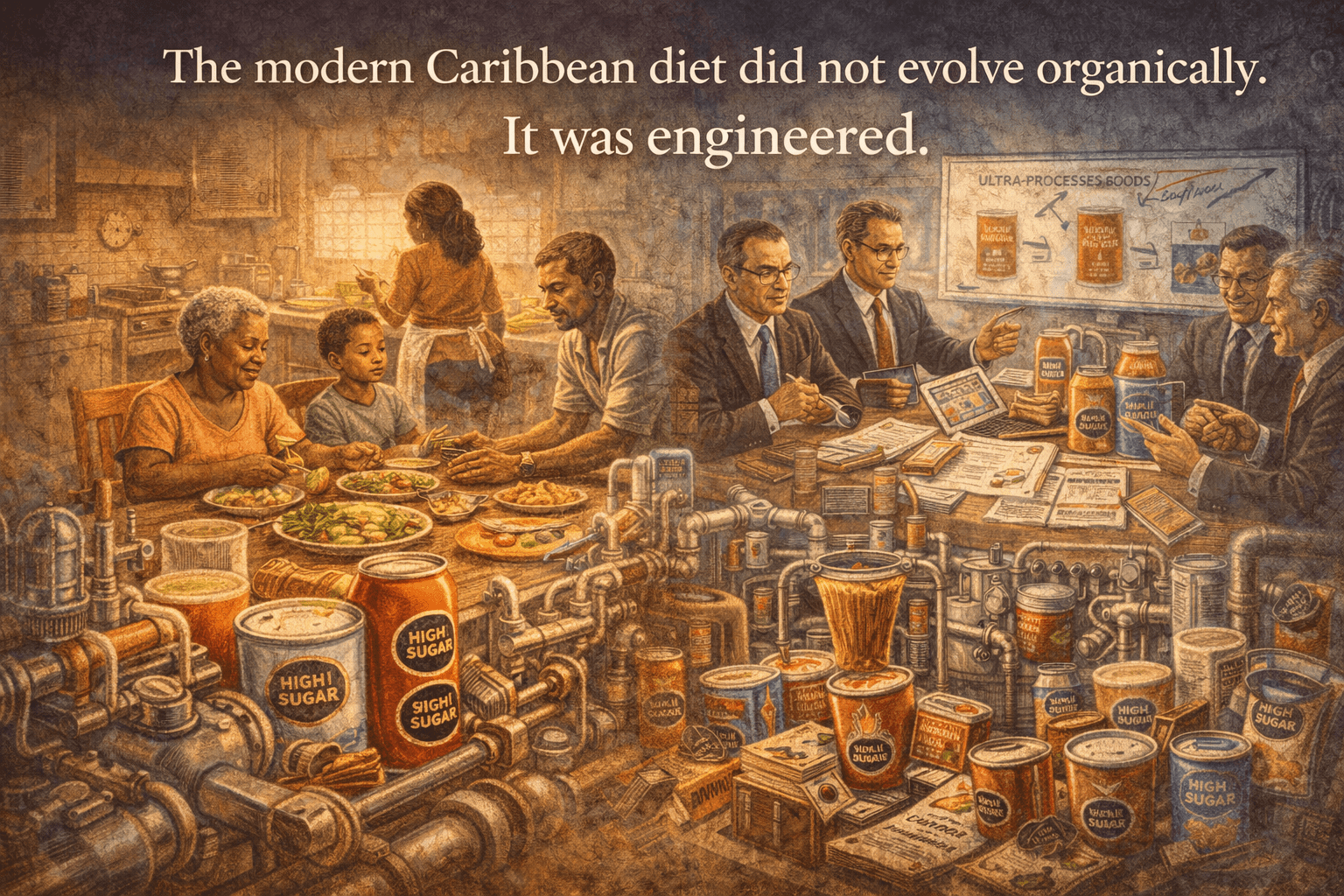
Historically, plantation diets emphasized cheap calories—salt, sugar, fat—to fuel labor. Today, trade liberalization has intensified that pattern.
Since the 1990s, imports of ultra-processed foods have surged. Following trade agreements with the United States, imports of frozen potatoes increased by over 70%. Today, more than 80% of food consumed in many Caribbean nations is imported, and a significant portion is highly processed.
These imports displaced traditional foods: legumes, ground provisions, fruits, and greens that sustained communities for generations.
Between 2006 and 2016, childhood obesity rates in parts of the Caribbean doubled.
This is not cultural failure. It is market displacement.
8. The Stigma of Survival: When Local Food Becomes “Poor Man’s Food”
Plantation logic also shapes perception.
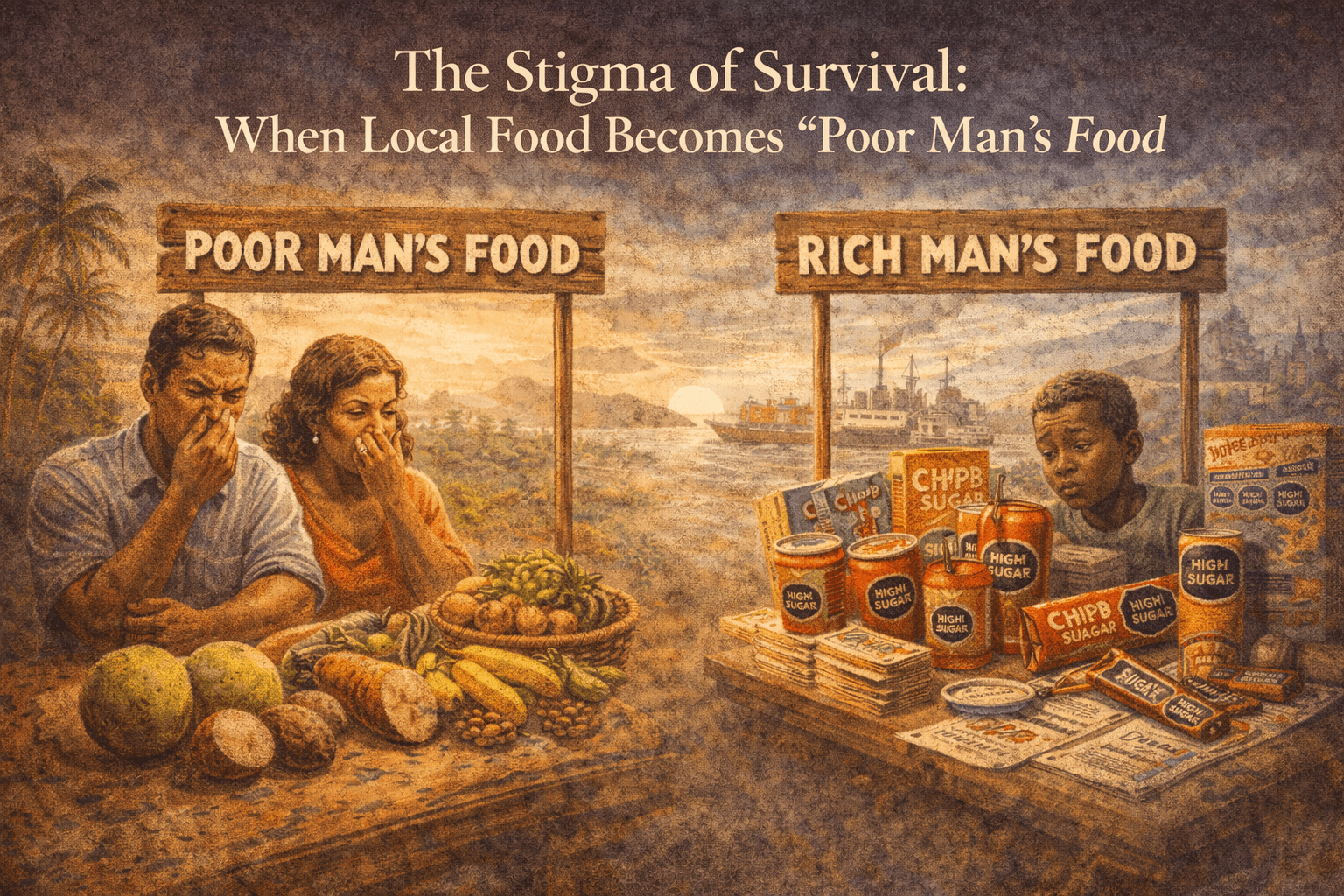
Foods that sustained Maroon communities—wild yams, bananas, bush meat, herbal preparations—are increasingly stigmatized as backward or inferior. Imported processed foods, by contrast, are associated with modernity, remittances, and status.
This inversion is not accidental.
It is the cultural residue of colonial trade hierarchies.
Reclaiming food sovereignty is not nostalgia.
It is health protection.
9. Climate, Heat, and Compounding Risk
The Caribbean is also confronting a new layer of stress: climate change.
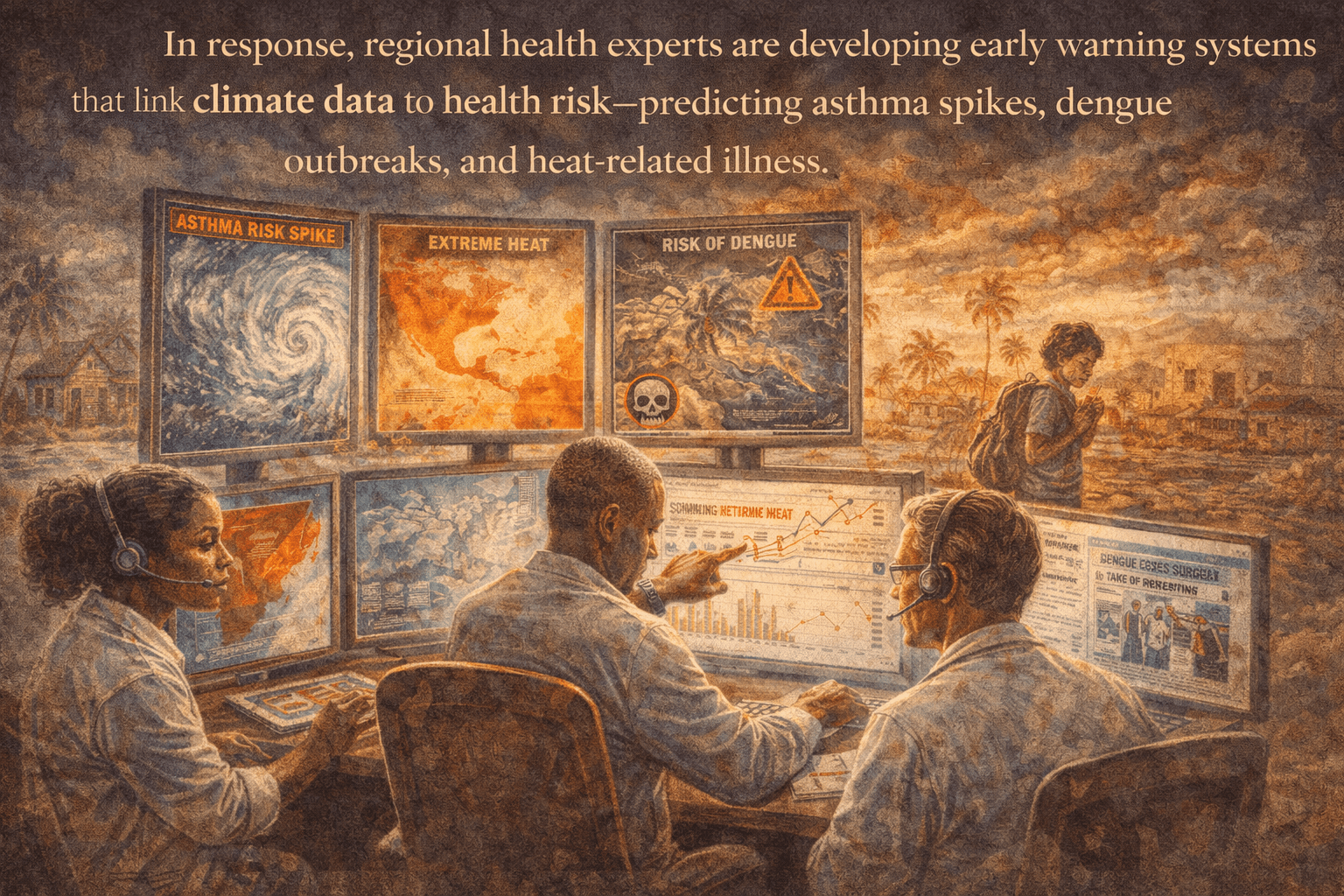
Rising temperatures, Sahara dust, and extreme weather events place additional strain on bodies already burdened by chronic disease. Heat exacerbates cardiovascular stress. Airborne dust worsens respiratory conditions. Food insecurity deepens after storms.
In response, regional health experts are developing early warning systems that link climate data to health risk—predicting asthma spikes, dengue outbreaks, and heat-related illness.
These systems demonstrate what prevention looks like when it is taken seriously.
They also raise a critical question:
Why is this level of foresight not applied to food systems?
10. The Global Warning
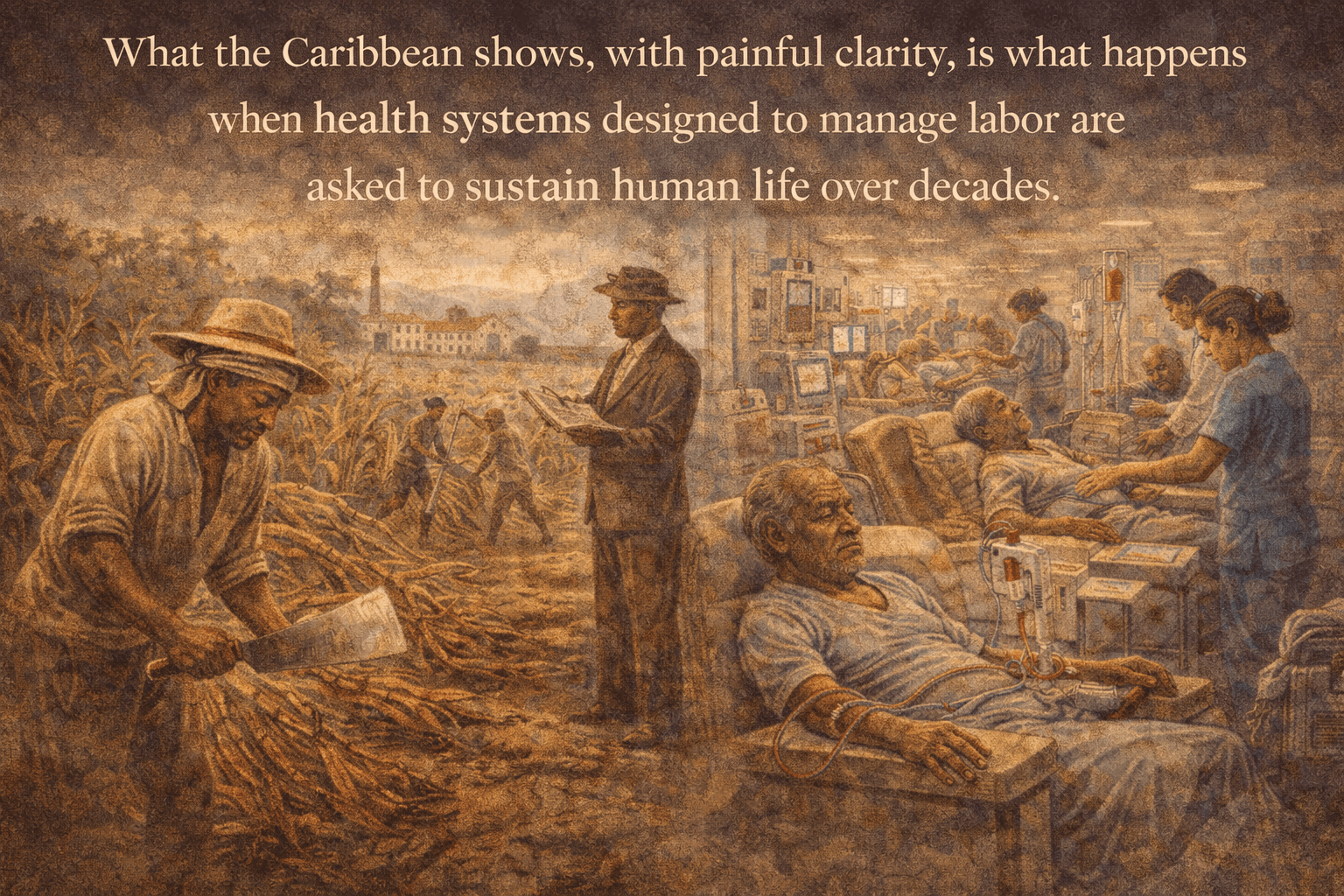
The Caribbean is not an outlier. It is a forecast.
The same patterns—late diagnosis, dialysis dependence, corporate interference, and trade-driven diets—are visible in Black communities across Canada, the UK, the United States, and Europe.
What the Caribbean shows, with painful clarity, is what happens when health systems designed to manage labor are asked to sustain human life over decades.
They fail.
Conclusion: Reclaiming the Caribbean Lifespan
Health is not a luxury, it is not a commodity, it is not a line item.,It is a human right.
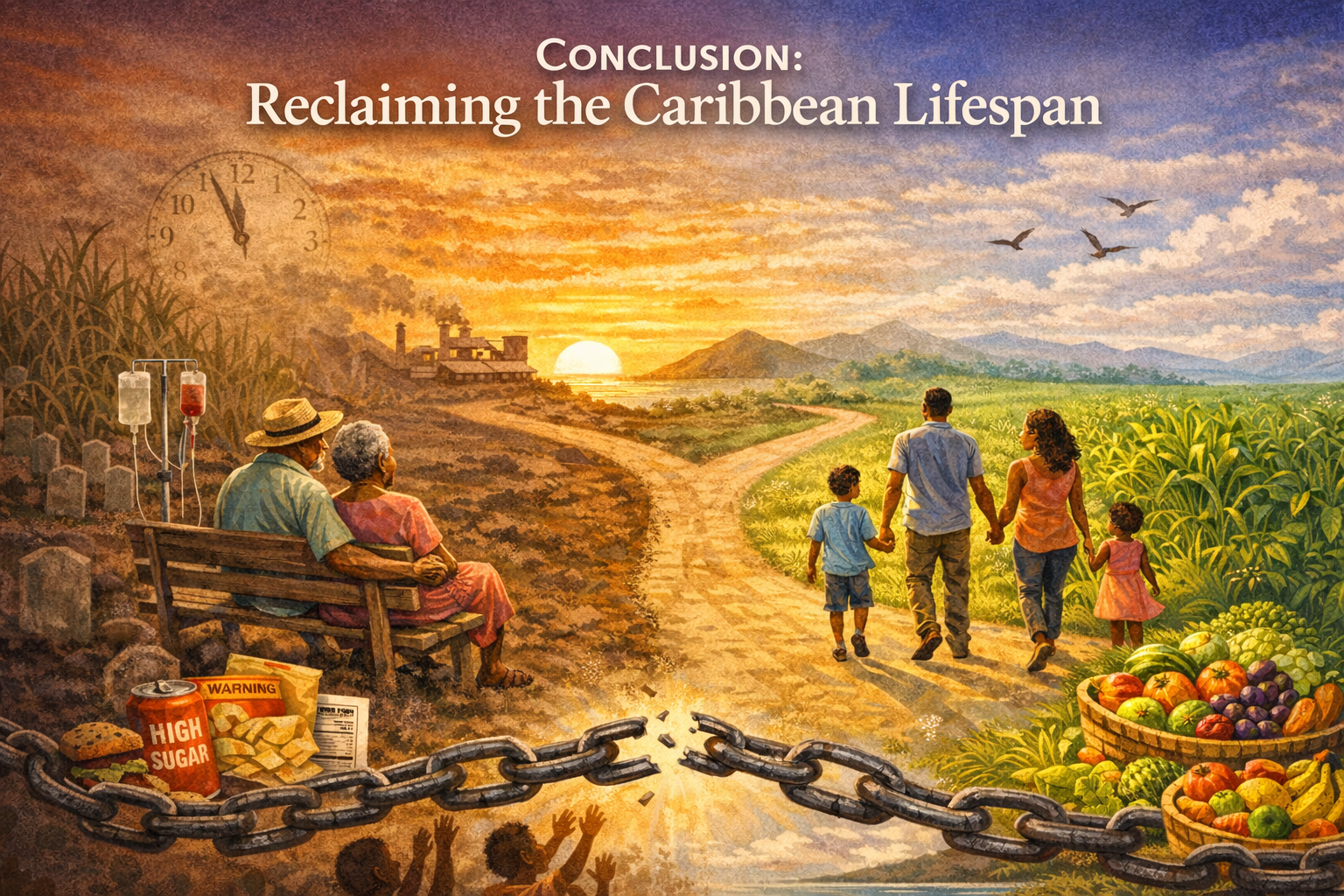
The fight for honest food labels is not about packaging. It is about time—time with our elders, time without dialysis machines, time to age with dignity.
The Caribbean stands at a crossroads. One path continues the logic of the plantation ledger: manage disease when bodies break. The other demands something different: prevention, accountability, and systems built to protect life.
If food labels are decided by the companies selling the products, who is protecting our children’s future?The stolen years are not gone yet. They can still be reclaimed.
Purpose of the Infographic
This infographic is designed to clearly explain why the Caribbean’s non-communicable disease (NCD) crisis is not just a regional issue, but a global warning. Its purpose is to shift understanding from individual behavior to system-level causes, showing how policy, trade, food systems, and health-care design shape long-term health outcomes.

What It Explains (Briefly)
The infographic walks readers through three connected ideas:
- The System – It shows how Caribbean health systems are often forced into crisis management, treating NCDs only after irreversible damage occurs, while prioritizing economic loss over human well-being.
- The Causes – It explains how trade liberalization, reliance on imported ultra-processed foods, high food costs, and modifiable risk factors (diet, inactivity, tobacco, alcohol, pollution) drive the NCD burden.
- The Prevention – It highlights evidence-based solutions, demonstrating that investing in prevention, primary care, food policy, and local agriculture delivers strong health and economic returns.
Overall, the infographic explains that the Caribbean’s experience reveals how global systems can quietly produce lifelong health crises—and how prevention-focused policy can change that trajectory.
Why Readers Should View This Presentation — and Why It Matters. PRESENTATION LINK: https://amhg.ca/wp-content/uploads/2026/02/2-Caribbean_Health_A_Roadmap_for_Resilience.pdf. Readers should view this presentation because it turns a complex, life-and-death issue into a clear, practical understanding. It explains how hypertension and maternal mortality are not isolated medical problems, but outcomes shaped by health systems, costs, policies, and access gaps—especially in Nigeria, where the global impact is profound. This presentation is important because it does three critical things at once:

- Reframes the problem from individual blame to system responsibility, showing why preventable deaths still occur.
- Provides protection-focused knowledge, including treatment gaps, medication safety, postpartum risks, and home monitoring—information that can save lives immediately.
- Connects maternal health to generational survival, demonstrating that protecting mothers is essential to protecting children, families, and the future of the global Black lifespan.
This is not just informative—it is empowering. It equips readers, families, and decision-makers with the insight needed to demand safer care, support prevention, and act before a crisis occurs.
Why This Video Matters
This video explains why food labels have become a critical line of defense for Caribbean and Black health. It shows how clear warning labels on sugar, salt, and fat empower families to make safer choices in a food system dominated by ultra-processed imports. VIDEO LINK: https://www.youtube.com/watch?v=bYaBndPznAE

VIDEO LINK : https://youtu.be/bYaBndPznAE
By connecting everyday shopping decisions to lifelong risks such as hypertension and diabetes, the video shows how simple policy tools can protect children, reduce preventable disease, and strengthen health across generations. Watching this video helps viewers understand that food labels are not about restriction—they are about protection, dignity, and safeguarding the Black lifespan.